


fig1
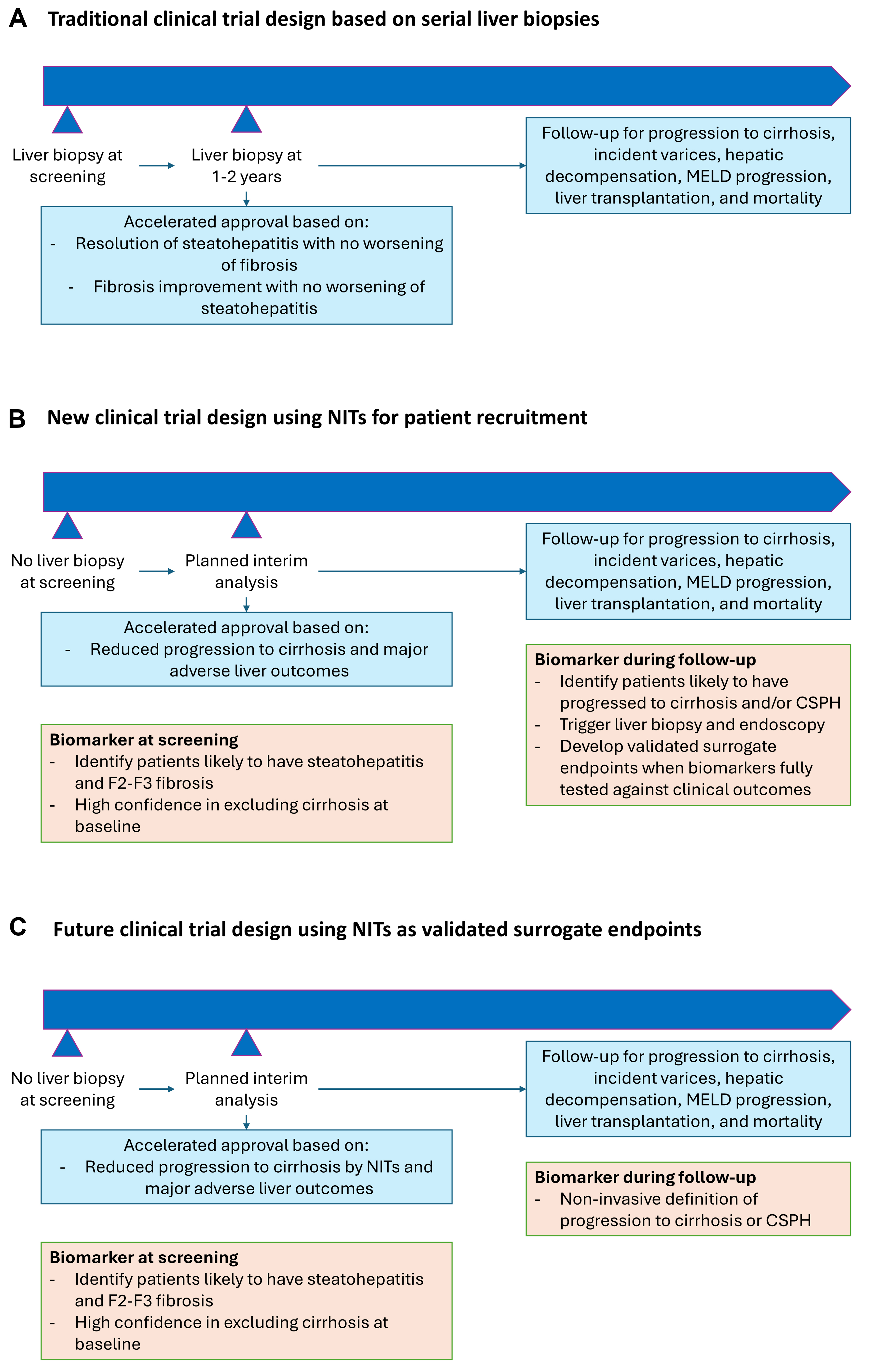
Figure 1. Evolution of clinical trial design for steatotic liver disease. (A) The traditional clinical trial design for MASH requires the use of serial liver biopsies for accelerated drug approval when MASH resolution and fibrosis improvement are achieved. The same trial or a separate trial is needed to demonstrate an improvement in “hard” clinical outcomes during long-term follow-up; (B) A new clinical trial design that can be applied to MASH and MetALD involves the use of NITs alone to identify patients with steatohepatitis and F2-F3 fibrosis, assuming that the tests are sufficient to exclude cirrhosis at baseline. During follow-up, in addition to collecting data on hepatic decompensation and liver-related death, NITs are used to identify patients who have likely progressed to cirrhosis. The latter is then confirmed by liver biopsy and can be counted as a clinical endpoint; (C) When one or more NITs have become validated surrogate endpoints, an entirely biopsy-free clinical trial design becomes possible. Drug approval can then depend solely on NIT response. CSPH: clinically significant portal hypertension; MELD: model for end-stage liver disease; MetALD: metabolic dysfunction-associated alcohol-related liver disease; MASH: metabolic dysfunction-associated steatohepatitis; NITs: noninvasive tests.





