


Open preperitoneal techniques: a bridge between anterior open and posterior endoscopic approaches
 0
0 Abstract
Mesh-based repair is the standard treatment for groin hernias. The HerniaSurge Group guidelines recommend both anterior open repair, such as the Lichtenstein repair, and minimally invasive posterior approaches including totally extraperitoneal repair (TEP) and transabdominal preperitoneal repair (TAPP). Over the past decades, several open preperitoneal techniques (OPPs) have been developed, combining posterior mesh placement with an open surgical approach. However, their role in contemporary hernia surgery remains underrecognized. This narrative review summarizes the historical development, anatomical rationale, and clinical evidence supporting OPPs, including transinguinal preperitoneal repair (TIPP), transrectus sheath preperitoneal repair (TREPP), open new simplified totally extraperitoneal repair (ONSTEP), and minimal open preperitoneal repair (MOPP). Preperitoneal mesh placement allows complete coverage of the myopectineal orifice, which represents the anatomical basis for modern posterior repairs. Registry analyses and comparative studies suggest that OPPs may be associated with lower rates of chronic postoperative pain compared with anterior repairs such as the Lichtenstein technique, while achieving outcomes comparable to those of endoscopic approaches. In addition, these techniques offer several practical advantages, including the possibility of performing the procedure under regional or local anesthesia, lower costs, and broad applicability across various clinical settings. OPPs represent a valuable intermediate option between anterior open and endoscopic repairs. By combining the anatomical advantages of posterior mesh placement with the simplicity of open surgery, they may be particularly useful in selected patients and in complex hernias. Greater recognition and further comparative studies are needed to better define their role in modern groin hernia surgery.
Keywords
INTRODUCTION
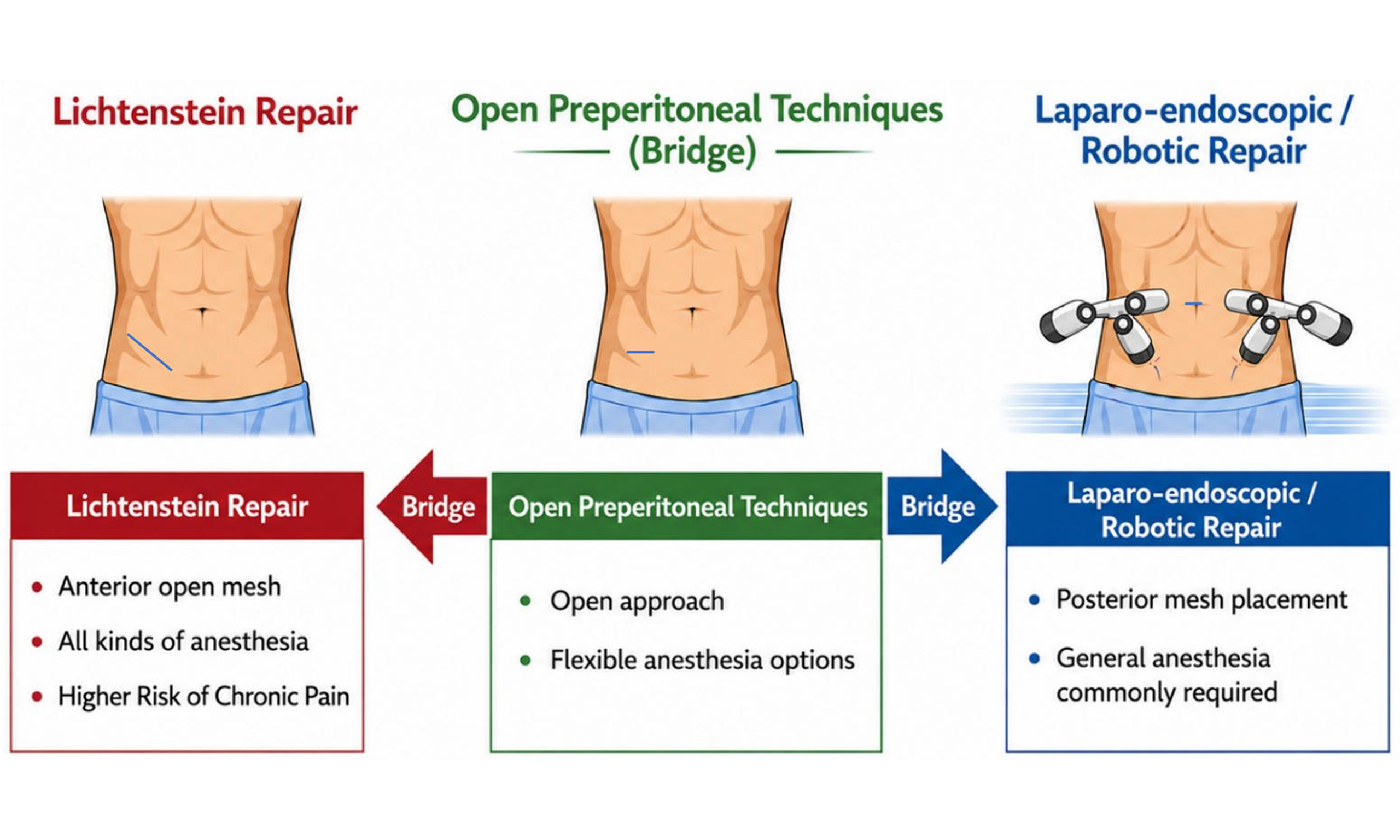
Groin hernia repair has undergone major technical evolution over recent decades, driven by advances in surgical techniques and prosthetic materials, leading to the widespread adoption of tension-free mesh repair as the current standard of care. Among open procedures, the Lichtenstein repair has long been regarded as the reference technique because of its simplicity, reproducibility, and low recurrence rates[1]. In parallel, posterior minimally invasive approaches, including totally extraperitoneal repair (TEP)[2,3] and transabdominal preperitoneal repair (TAPP)[4,5], have gained increasing popularity, particularly because of reduced postoperative pain and faster recovery. Current international guidelines from the HerniaSurge Group recommend a tailored approach based on patient characteristics, surgeon expertise, and available resources, considering both anterior open mesh repair and posterior endoscopic repair as valid strategies[6,7]. However, this traditional dichotomy between “open” and “laparoscopic” approaches may overlook a more fundamental consideration: the position of the prosthetic mesh relative to the myopectineal orifice. This raises an important question: should groin hernia repair be primarily considered in terms of surgical access, or rather in relation to the anatomical plane of mesh placement? Posterior mesh placement in the preperitoneal space allows complete coverage of this region and represents a key principle in modern hernia repair. This concept underlies not only endoscopic techniques but also a group of contemporary open procedures collectively referred to in this review as open preperitoneal techniques (OPPs). These include the pioneering gridiron preperitoneal approach described by Ugahary[8] and its modern evolutions, including transinguinal preperitoneal repair (TIPP)[9], transrectus sheath preperitoneal repair (TREPP)[10], open new simplified totally extraperitoneal repair (ONSTEP)[11], and minimal open preperitoneal repair (MOPP)[12]. The acronym OPPs is used throughout this review as a collective term for modern OPPs that combine limited open access with posterior mesh placement. Rather than maintaining a strict opposition between “open” and “laparoscopic” approaches, groin hernia repair may be more appropriately viewed as a continuum of techniques sharing common anatomical principles, within which OPPs occupy a distinct position. This perspective shifts the paradigm from a purely technical classification toward an anatomically driven approach. Despite encouraging clinical outcomes and growing interest among specialized hernia surgeons, OPPs remain less widely adopted than either the Lichtenstein repair or endoscopic approaches. In current practice, “open” repair commonly refers to anterior techniques such as Lichtenstein, whereas “minimally invasive” approaches generally denote laparo-endoscopic and robotic posterior repairs. The aim of this review is to discuss the historical development, anatomical rationale, and current evidence supporting OPPs, with particular emphasis on their role as an intermediate and complementary option between anterior open repair and posterior endoscopic approaches, especially in selected patients and complex clinical scenarios.
HISTORICAL DEVELOPMENT OF PREPERITONEAL REPAIR
The evolution of preperitoneal repair in groin hernia surgery reflects the progressive integration of anatomical knowledge and advances in prosthetic materials. A major milestone in the understanding of groin hernias was the description of the myopectineal orifice by Henri Fruchaud, who demonstrated that indirect, direct, and femoral hernias arise from a common anatomical area of weakness. This observation profoundly influenced the conceptual approach to groin hernia repair[13]. The development of synthetic prosthetic materials in the mid-twentieth century marked another key step in the evolution of hernia surgery. Usher introduced the clinical use of polypropylene mesh, enabling tension-free reinforcement of the abdominal wall[14]. Around the same period, Nyhus et al. advocated the preperitoneal approach as a rational method for groin hernia repair, emphasizing posterior reinforcement of the abdominal wall[15]. Building on these concepts, European surgeons such as Jean Rives and René Stoppa further developed techniques based on the placement of large prosthetic meshes within the preperitoneal space. Their work demonstrated that broad prosthetic reinforcement of the entire groin region could effectively prevent the development of new groin hernias[16]. In the early 1990s, the advent of endoscopic surgery led to the widespread adoption of posterior mesh placement through techniques such as TEP[2,3] and TAPP[4,5]. These approaches confirmed the effectiveness of preperitoneal mesh reinforcement and contributed to renewed interest in posterior repair strategies. Subsequently, several surgeons sought to reproduce these posterior principles through simplified open access to the preperitoneal space. Ugahary described a minimal open approach using a grid-iron incision to reach the preperitoneal plane[8], which influenced the development of contemporary OPPs. These include TIPP, TREPP, ONSTEP, and, more recently, MOPP has been introduced as an open technique designed to combine posterior mesh reinforcement with a limited surgical approach and specialized instrumentation. Although these techniques differ in their surgical access and technical details, they share the same fundamental objective: reinforcement of the groin through mesh placement within the preperitoneal space. These contemporary OPPs represent the modern evolution of this concept and constitute the focus of the present review.
ANATOMICAL RATIONALE FOR PREPERITONEAL MESH REPAIR
A central principle in groin hernia surgery is the need to reinforce the entire myopectineal orifice rather than simply closing the visible hernia defect. Because indirect, direct, and femoral hernias all arise from this anatomical region, repairing only the apparent defect may fail to address the underlying anatomical weakness[13].
Preperitoneal mesh placement directly addresses this limitation. When a prosthetic mesh is positioned within the preperitoneal plane, it ensures comprehensive reinforcement of this region, covering all potential hernia sites. In addition, the preperitoneal location allows the mesh to benefit from intra-abdominal pressure, which presses the prosthesis against the abdominal wall and contributes to its stabilization. This mechanical effect enhances the effectiveness of posterior repairs and may allow mesh placement without the need for fixation. Another important advantage relates to the relationship between the prosthesis and the inguinal nerves. In anterior repairs such as the Lichtenstein technique, the mesh is placed within the inguinal canal in close proximity to the ilioinguinal, iliohypogastric, and genital branch of the genitofemoral nerves. This anatomical configuration has been associated with chronic postoperative pain, one of the most significant long-term complications following groin hernia repair. In contrast, preperitoneal mesh placement avoids contact with the major inguinal nerves, as the prosthesis is positioned in a plane where these nerves are not encountered. This anatomical separation may reduce the risk of nerve-related postoperative pain[17]. The posterior approach also provides improved visualization of the entire inguinofemoral region, facilitating the identification of multiple or occult hernia defects, including femoral hernias that may be overlooked during anterior repairs. These anatomical and biomechanical features together provide a strong anatomical and functional rationale for preperitoneal mesh placement in modern groin hernia repair.
CURRENT OPPS
Over the past two decades, several open surgical techniques have been developed to enable mesh placement within the preperitoneal space while preserving the advantages of an open approach. Although these procedures differ in their surgical access and technical details, they share the same objective: comprehensive reinforcement of the groin through posterior mesh placement. The main techniques currently described include TIPP, TREPP, ONSTEP, and MOPP.
TIPP places a prosthetic mesh in the preperitoneal space through the inguinal canal. Early development of the transinguinal preperitoneal concept was described by Pélissier, who reported preperitoneal placement of a memory-ring patch through an anterior approach[9], before the term TIPP became widely adopted. This approach allows surgeons familiar with anterior groin anatomy to access the posterior plane while maintaining a limited incision and a technique closely related to conventional open hernia repair. The procedure has been adopted in several European centers and has demonstrated encouraging outcomes in registry analyses and comparative studies.
TREPP represents a pure posterior open approach, providing direct access to the preperitoneal plane through a short supra-inguinal incision[9]. By approaching the posterior space through the rectus sheath, the technique avoids dissection within the inguinal canal and enables a repair conceptually similar to endoscopic procedures.
ONSTEP represents a simplified variation within the OPPs family[11]. In this technique, access to the preperitoneal space and medial dissection are performed in a manner similar to other approaches, but without parietalization of the spermatic cord structures. A specially designed mesh is positioned partly in the preperitoneal space and partly in the intermuscular plane, allowing broad posterior coverage while simplifying the operative steps.
MOPP has been introduced as a minimal open approach to preperitoneal mesh placement. The technique builds on principles described by Franz Ugahary, using specific atraumatic retractors to facilitate gentle access to the preperitoneal space through the deep inguinal ring. Entry into the preperitoneal plane is guided by anatomical landmarks, particularly the transversalis fascia, which serves both as a reference for accessing the posterior space and for initiating parietalization of the spermatic cord in medial hernias. Further technical details of this technique have been reported in a dedicated publication[12].
Despite differences in surgical access, these techniques share several common features, including creation of a preperitoneal working space, placement of a large mesh ensuring broad coverage of the groin, and limited or absent mesh fixation. Their outcomes therefore appear to depend primarily on the principle of posterior reinforcement rather than on the specific approach used. Comparative results with Lichtenstein repair and endoscopic techniques are discussed in the following sections. The main surgical approaches among OPPs are summarized in Table 1.
Comparison of surgical approaches for primary groin hernia repair
| Approach group | Technique | Surgical access | Mesh position | Anesthesia | Learning curve | Cost | Main advantages | Main limitations |
| Anterior | Lichtenstein | Anterior (conventional incision) | Anterior | Local/regional/GA | Short | low | Simple, reproducible | Higher chronic pain risk; incomplete MPO coverage |
| OPPs | TIPP/MOPP | Anterior (minimal incision) | Preperitoneal | Local/regional/GA | Moderate | Low-moderate | Large preperitoneal mesh via minimal incision | Limited in severe obesity |
| TREPP/Ugahary | Posterior (minimal incision) | Preperitoneal | Local/regional/GA | Moderate-long | Low-moderate | Direct posterior access | Limited in severe obesity | |
| ONSTEP | Anterior (minimal incision) | Dual-plane (preperitoneal and intermuscular) | Local/regional/GA | Short | Low-moderate | Simplified dual-plane repair | Limited in severe obesity | |
| Endoscopic | TEP/TAPP/robotic | Posterior (endoscopic access) | Preperitoneal | General anesthesia, endotracheal intubation, neuromuscular blockade | Long (TEP); moderate (TAPP, robotic) | High (TEP/TAPP); very high (robotic) | Excellent visualization; full MPO coverage | Less suitable for frail patients; complex hernias |
OPPS VS. LICHTENSTEIN REPAIR
The Lichtenstein repair remains one of the most widely performed operations for inguinal hernia repair worldwide[18]. Its popularity is largely due to its technical simplicity, reproducibility, and low recurrence rates. However, the anterior placement of the prosthetic mesh within the inguinal canal has raised concerns regarding chronic postoperative pain. In clinical practice, anterior open repair is often selected in situations where laparo-endoscopic approaches are considered unsuitable, such as in elderly or frail patients or in the presence of large or complex hernias. In this context, Lichtenstein repair frequently represents the default open option[6,7]. Several studies have suggested that the position of the mesh may play a key role in postoperative outcomes. In anterior repairs such as Lichtenstein, the prosthesis is placed in close proximity to the ilioinguinal and iliohypogastric nerves, as well as the genital branch of the genitofemoral nerve, which may contribute to nerve irritation and chronic postoperative pain[17]. In contrast, OPPs place the mesh in the preperitoneal plane, where the major inguinal nerves are not encountered, thereby reducing the potential for mesh–nerve interaction[19]. Registry-based analyses comparing different techniques have provided further insight into this issue. Data from large hernia registries have shown significantly lower rates of chronic postoperative pain after TIPP compared with Lichtenstein repair[7,19]. Beyond pain outcomes, the anatomical characteristics of preperitoneal repair may also improve the completeness of the repair. By providing broad coverage of the entire groin region, posterior repairs allow simultaneous reinforcement of the direct, indirect, and femoral areas, and may reduce the risk of unrecognized femoral defects that can occasionally be overlooked during anterior inguinal repairs. OPPs may offer an alternative in these situations, combining the advantages of an open approach, such as a limited incision and the possibility of regional or local anesthesia, with the anatomical benefits of posterior mesh placement. As a result, these techniques may represent a relevant option in situations where Lichtenstein repair is traditionally performed, while providing additional anatomical and functional advantages [Table 1].
OPPS VS. LAPARO-ENDOSCOPIC AND ROBOTIC REPAIR
Laparo-endoscopic posterior repairs, particularly TEP and TAPP, have gained widespread acceptance in modern groin hernia surgery. These techniques are based on principles established by earlier preperitoneal repairs, namely placement of a prosthetic mesh in the preperitoneal space to achieve broad reinforcement of the groin region. However, laparo-endoscopic repair requires general anesthesia, specialized equipment, and a significant learning curve, which may limit its broader adoption in certain healthcare systems or in centers where advanced minimally invasive training is not readily available. More recently, robotic-assisted techniques have emerged as a technological extension of endoscopic surgery. Robotic platforms offer improved ergonomics, enhanced three-dimensional visualization, and greater instrument articulation, which may facilitate dissection and mesh placement, particularly in technically demanding situations[20]. Nevertheless, comparative studies and meta-analyses generally report similar clinical outcomes between robotic and conventional laparo-endoscopic repair[21]. In addition, robotic procedures are associated with substantially higher costs[22], which continues to limit their widespread use for a common condition such as groin hernia. In clinical practice, both laparo-endoscopic and robotic repairs may be avoided in certain situations, including frail patients, large inguinoscrotal hernias, or recurrences after previous laparo-endoscopic repair. In these circumstances, surgeons frequently resort to open techniques[7,23]. In this setting, OPPs provide a relevant alternative by allowing posterior mesh placement through an open approach. Evidence from registry-based analyses in large inguinoscrotal hernias suggests that techniques such as MOPP can achieve outcomes comparable to both Lichtenstein and laparo-endoscopic repair, with favorable outcomes in terms of postoperative pain and recovery[24]. OPPs represent an alternative way to achieve posterior mesh placement without the need for pneumoperitoneum or advanced laparoscopic instrumentation. Comparative studies and registry analyses have suggested that outcomes following techniques such as TIPP are comparable to those of laparo-endoscopic approaches in terms of recurrence and chronic postoperative pain[19]. Another important advantage of OPPs is the flexibility of anesthesia. While laparo-endoscopic procedures are predominantly performed under general anesthesia and may be associated with airway control and neuromuscular blockade, OPPs can often be performed under general anesthesia using a laryngeal mask without neuromuscular blockade, or under regional, and in selected cases by appropriately trained surgeons, even under local anesthesia. Although selected laparo-endoscopic repairs may also be performed without general anesthesia, this remains uncommon in routine practice. This characteristic may be particularly advantageous in elderly patients or in individuals with significant comorbidities who may not tolerate general anesthesia with pneumoperitoneum[6].
In this context, the conventional distinction between “open” and “minimally invasive” repair may be overly simplistic. In practice, the overall invasiveness of a procedure depends on multiple factors, including the type of anesthesia, physiological stress, and technical complexity, rather than on the surgical access alone [Table 1].
CLINICAL INDICATIONS FOR OPPS
In contemporary groin hernia surgery, the choice of operative technique should follow a tailored approach based on patient characteristics, hernia morphology, and surgeon expertise. Within this framework, OPPs may represent a valuable option in several specific clinical scenarios[6,7]. One important indication concerns elderly or frail patients with significant comorbidities. In daily practice, laparo-endoscopic repair is often avoided in such patients because of the need for general anesthesia and pneumoperitoneum, leading many surgeons to select an anterior open repair such as the Lichtenstein technique[6]. OPPs offer an alternative in this setting, as they allow posterior mesh placement while maintaining limited surgical access and the possibility of regional or local anesthesia. This combination may represent a particularly relevant option in patients who are not ideal candidates for laparo-endoscopic surgery. OPPs may also be advantageous in the management of large or complex groin hernias, including large direct defects, combined hernias, and inguinoscrotal hernias[24]. In these situations, endoscopic dissection may be technically demanding, and anterior repair is frequently preferred. However, OPPs allow broad coverage of the groin region through a direct and controlled approach, which may be particularly well suited to these complex presentations. Recurrent hernia after a previous anterior repair may also represent an indication for OPPs. However, the feasibility in this setting depends on the specific technique used. Approaches that access the preperitoneal plane outside the inguinal canal, such as the original Ugahary approach or the TREPP technique, allow relatively straightforward dissection in a previously unoperated plane. In contrast, transinguinal techniques such as TIPP, MOPP, or ONSTEP may be less suitable in this context because of scarring within the inguinal canal. Careful selection of the surgical approach is therefore required[11].
Finally, OPPs may represent a pragmatic option in healthcare environments where laparo-endoscopic equipment or expertise is limited. Because these procedures rely on standard surgical instruments and relatively straightforward operative steps, they allow application of posterior repair principles without the logistical and economic constraints associated with laparoscopic or robotic surgery.
Taken together, these considerations suggest that OPPs occupy an intermediate and complementary option between anterior open and laparo-endoscopic approaches. In particular, they may provide a relevant option in situations where laparoscopy is not feasible, while avoiding the limitations associated with anterior mesh placement. The respective indications of anterior open, OPPs, and laparo-endoscopic approaches according to clinical scenarios are summarized in Table 2.
Comparative surgical indications of Lichtenstein techniques, open pre peritoneal techniques, endoscopic/robotic techniques
| Clinical scenario | Lichtenstein | MOPP | TIPP | TREPP/Ugahary | ONSTEP | Endoscopic/robotic |
| Primary uncomplicated groin hernia | Suitable | Suitable | Suitable | Suitable | Selected cases (non-obese, small/medium) | Suitable |
| Recurrent hernia after previous anterior repair | Not recommended | Not recommended | Not recommended | Preferred | Less suitable | Preferred |
| Recurrent hernia after previous posterior repair | Preferred | Not recommended | Not recommended | Not recommended | Not recommended | Not recommended |
| Large direct/combined/primary hernia | Suitable | Suitable | suitable | Suitable | Less suitable | Suitable |
| Primary inguinoscrotal hernia | Suitable | Possible with expertise | Possible with expertise | Possible with expertise | Not recommended | Less suitable |
| Very frail/high anesthetic risk patient | Suitable | Suitable | Suitable | Suitable | Suitable | Not recommended |
| Obesity/morbid obesity | Suitable | Less suitable | Less suitable | Less suitable | Least suitable | Preferred |
| Anesthesia flexibility | High (local/regional possible) | High (local/regional possible) | High (local/regional possible) | High (local/regional possible) | High (local/regional possible) | Low (general anesthesia + neuromuscular blockade required) |
LIMITATIONS OF OPPS
Despite their potential advantages, OPPs present several limitations that should be carefully considered. First, most of the available evidence originates from specialized hernia centers or surgeons with significant experience in preperitoneal dissection. As a result, the reproducibility of these techniques in general surgical practice remains to be fully established, and outcomes may depend on appropriate training and case selection. Second, OPPs do not represent a single standardized technique, but rather a group of approaches with different operative pathways and technical nuances. This heterogeneity may contribute to variability in outcomes and may complicate comparisons between studies. Third, the surgical management of recurrence may differ depending on the technique used. In transinguinal approaches such as TIPP, MOPP, or ONSTEP, both the inguinal canal and the preperitoneal space are dissected, which may complicate reoperations in the event of recurrence. In contrast, techniques that access the preperitoneal plane outside the inguinal canal, such as the Ugahary approach or TREPP, preserve an undisturbed anterior plane, allowing a more straightforward anterior repair if needed. Overall, recurrence rates remain low when these techniques are performed by experienced surgeons. Fourth, the learning curve associated with preperitoneal dissection should not be underestimated. These procedures may be technically more demanding when performed through a limited-access incision and require a precise understanding of posterior anatomy as well as meticulous dissection. Technical challenges may arise during both access to and dissection of the preperitoneal space, as well as during adequate parietalization of the spermatic cord, which are essential steps for proper mesh deployment.
Fifth, some OPPs rely on prosthetic meshes specifically designed to facilitate deployment through a limited incision. The availability and cost of these devices may vary across healthcare systems, potentially limiting broader adoption.
Finally, the current evidence supporting OPPs remains heterogeneous. Randomized evidence is available for TIPP through the TULIP trial[25], while additional comparative evidence has been provided for TREPP through propensity-score-matched analyses[26]. Together, these studies have contributed valuable information regarding postoperative pain and long-term outcomes. However, most published data still originate from observational studies, registry analyses, or specialized centers with substantial experience in OPPs. Consequently, the generalizability of these results to broader surgical practice remains to be fully established. Further comparative studies involving a wider range of surgeons and clinical settings would help to better define the role of OPPs in contemporary groin hernia surgery.
Taken together, these limitations highlight the importance of surgical expertise, appropriate technical execution, and wider dissemination of standardized approaches when considering OPPs.
CONCLUSION
OPPs represent a relevant and underrecognized option in contemporary groin hernia repair. By combining an open surgical approach with preperitoneal mesh placement, they integrate key features of both anterior open and posterior endoscopic approaches. In selected clinical situations, they may represent a valuable alternative not only when laparo-endoscopic repair is not feasible, but also to anterior open techniques such as the Lichtenstein repair, by providing the anatomical advantages of posterior mesh placement while preserving the simplicity of an open approach. Further studies are needed to better define their role and optimize their integration into tailored surgical strategies.
DECLARATIONS
Acknowledgments
The author would like to acknowledge the French Hernia Club (Club Hernie) and its members for their longstanding contribution to clinical research and education in abdominal wall surgery. Many of the studies cited in this review originated from collaborative work within the Club Hernie and from analyses based on the Club Hernie Registry. The author is particularly grateful to Dr. Jean-François Gillion, President of the Club Hernie, for his invaluable assistance in the development and management of the Club Hernie Registry database.
Authors’ contributions
The author contributed solely to the article.
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool ChatGPT (OpenAI, GPT-5.5, released on 2026-04-23) was used solely for English language editing, improving the clarity and consistency of the manuscript, and the preparation of the Graphic Abstract. The AI tool did not influence the scientific content, study design, interpretation of the literature, or the conclusions of this review. The author directed and approved all modifications, reviewed the final version in its entirety, and assumes full responsibility for the scientific content, terminology, graphical presentation, and final editorial decisions.
Financial support and sponsorship
None.
Conflicts of interest
The author declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Amid PK. Lichtenstein tension-free hernioplasty: its inception, evolution, and principles. Hernia. 2004;8:1-7.
2. Dulucq JL. Treatment of inguinal hernias by placement of a preperitoneal prosthetic patch using the totally extraperitoneal approach. Cahiers de Chir. 1991;79:15-6.
3. Ferzli GS, Massad A, Albert P. Extraperitoneal endoscopic inguinal hernia repair. J Laparoendosc Surg. 1992;2:281-6.
4. Arregui ME, Davis CJ, Yucel O, Nagan RF. Laparoscopic mesh repair of inguinal hernia using a preperitoneal approach: a preliminary report. Surg Laparosc Endosc. 1992;2:53-8.
5. Leroy J, Fromont G. Adult groin hernias: preperitoneal prosthetic repair under laparoscopic guidance (report of 110 cases). J Coelio Chir. 1992;1:22-5.
7. Stabilini C, van Veenendaal N, Aasvang E, et al. Update of the international HerniaSurge guidelines for groin hernia management. BJS Open. 2023;7:zrad080.
8. Ugahary F. The Gridiron Hernioplasty. In: Bendavid R, Abrahamson J, Arregui ME, Flament JB, editors. Abdominal wall hernias principles and management. New York: Springer; 2001. pp. 407-11.
9. Pélissier EP. Inguinal hernia: preperitoneal placement of a memory-ring patch by anterior approach. Preliminary experience. Hernia. 2006;10:248-52.
10. Akkersdijk WL, Andeweg CS, Bökkerink WJ, Lange JF, van Laarhoven CJ, Koning GG. Teaching the transrectus sheath preperitoneal mesh repair: TREPP in 9 steps. Int J Surg. 2016;30:150-4.
11. Lourenço A, da Costa RS. The ONSTEP inguinal hernia repair technique: initial clinical experience of 693 patients, in two institutions. Hernia. 2013;17:357-64.
12. Soler M. The minimal open preperitoneal (MOPP) approach for treating groin hernias: technique, indications, and results. Ann Laparosc Endosc Surg. 2024;9:3-3.
13. Fruchaud H. Anatomie chirurgicale des hernies de l’aine. Paris: Masson; 1956. Available from: https://books.google.com/books/about/Anatomie_chirurgicale_des_hernies_de_l_a.html?id=ycSfqul2ViMC. [Last accessed on 10 Jul 2026].
14. Usher FC. Knitted Marlex mesh. An improved Marlex prosthesis for repairing hernias and other tissue defects. Arch Surg. 1961;82:771-3.
15. Nyhus LM, Condon RE, Harkins HN. Clinical experiences with preperitoneal hernial repair for all types of hernia of the groin, with particular reference to the importance of transversalis fascia analogues. Am J Surg. 1960;100:234-44.
16. Stoppa RE, Rives JL, Warlaumont CR, Palot JP, Verhaeghe PJ, Delattre JF. The use of Dacron in the repair of hernias of the groin. Surg Clin North Am. 1984;64:269-85.
17. Poobalan AS, Bruce J, King PM, Chambers WA, Krukowski ZH, Smith WC. Chronic pain and quality of life following open inguinal hernia repair. Br J Surg. 2001;88:1122-6.
18. Messias BA, de Almeida PL, Ichinose TMS, et al. The Lichtenstein technique is being used adequately in inguinal hernia repair: national analysis and review of the surgical technique. Rev Col Bras Cir. 2023;50:e20233655.
19. Hurel R, Bouazzi L, Barbe C, et al.; Club-Hernie members. Lichtenstein versus TIPP versus TAPP versus TEP for primary inguinal hernia, a matched propensity score study on the French Club Hernie Registry. Hernia. 2023;27:1165-77.
20. Xie J, Koo DC, Lee MJ, Sugiyama G. The evolution of minimally invasive inguinal hernia repairs. Ann Laparosc Endosc Surg. 2024;9:13.
21. Solaini L, Cavaliere D, Avanzolini A, Rocco G, Ercolani G. Robotic versus laparoscopic inguinal hernia repair: an updated systematic review and meta-analysis. J Robot Surg. 2022;16:775-81.
22. Hinojosa-Ramirez F, Tallon-Aguilar L, Tinoco-Gonzalez J, et al. Economic analysis of the robotic approach to inguinal hernia versus laparoscopic: is it sustainable for the healthcare system? Hernia. 2024;28:1205-14.
23. Tran HM, MacQueen I, Chen D, Simons M. Systematic review and guidelines for management of scrotal inguinal hernias. J Abdom Wall Surg. 2023;2:11195.
24. Gillion JF, Soler M, Mettoudi A, et al.; Club-Hernie Members. Three-arm registry-based comparison of trans-inguinal-pre-peritoneal, laparoscopic, and Lichtenstein techniques for scrotal hernia repair. J Abdom Wall Surg. 2025;4:13993.
25. Bökkerink WJV, Koning GG, Malagic D, van Hout L, van Laarhoven CJHM, Vriens PWHE. Long-term results from a randomized comparison of open transinguinal preperitoneal hernia repair and the Lichtenstein method (TULIP trial). Br J Surg. 2019;106:856-61.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].