


Rare indications for transanal endoscopic microsurgery
 0
0 Abstract
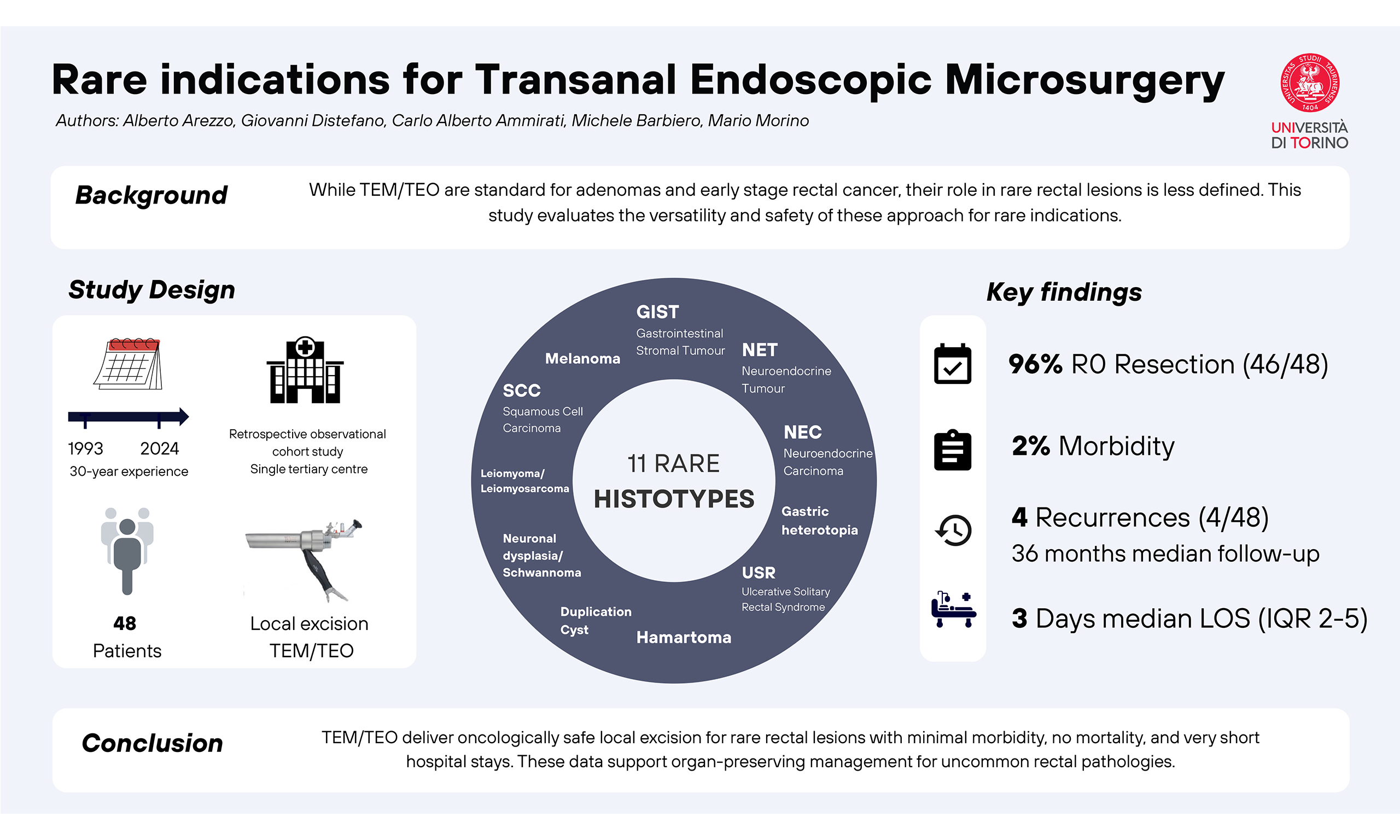
Aim: Transanal endoscopic microsurgery (TEM) and transanal endoscopic operation (TEO) are enabling platforms for tailored full-thickness or submucosal rectal excision. We evaluated outcomes of patients with rare rectal indications managed using these platforms.
Methods: We performed a single-centre retrospective cohort study of consecutive patients treated with TEM or TEO between 1993 and 2024 for lesions with rare final rectal histology. Inclusion criteria were local excision by TEM/TEO, rare definitive histology, and available perioperative data; standard indications (adenoma/adenocarcinoma), non-rectal lesions, and incomplete records were excluded. Data included lesion characteristics, operative details, margins, complications, hospital stay, follow-up, and recurrence.
Results: Forty-eight patients across 11 histotype groups were included. Excision was full-thickness in 45/48 cases and submucosal in 3/48. Peritoneal entry occurred in 3/48 and was managed on-platform without conversion. R0 resection was achieved in 46/48 patients. Four postoperative complications occurred overall; only one bleeding episode required transfusion and reoperation. There was no mortality. Median length of stay was 3 days [interquartile range (IQR), 2-5], and median follow-up was 36 months (IQR, 22-49). Recurrence occurred in 4/48 patients.
Conclusions: TEM/TEO provided safe, organ-preserving local excision for rare rectal lesions, with high R0 rates, limited morbidity, no mortality, and short hospital stay. These data support the use of rigid transanal endoscopic platforms for selected uncommon rectal pathologies.
Keywords
INTRODUCTION
Transanal endoscopic microsurgery (TEM), introduced by Buess in the 1980s, and its successor, the transanal endoscopic operation (TEO), have profoundly expanded the armamentarium of minimally invasive rectal surgery[1]. These rigid platforms provide a stable pneumorectum, magnified stereoscopic vision, and a dedicated set of instruments that enable precise excision of rectal lesions. Although initially conceived for benign adenomas and early-stage rectal carcinoma, the platforms have progressively been applied to a much broader spectrum of rectal conditions. Their versatility lies not in a single procedure but in their role as enabling platforms upon which various dissection strategies can be executed, including full-thickness resections and submucosal dissections. This adaptability allows TEM and TEO to address a range of rare rectal pathologies that were once the domain of radical resection or managed suboptimally by conventional transanal excision[2].
The core advantages of TEM and TEO derive from their capacity to overcome the inherent limitations of traditional transanal surgery. Conventional transanal excision is limited by poor exposure, a restricted working distance, and inadequate instrumentation, factors that collectively compromise the oncological adequacy of resections, particularly for more proximal or larger lesions[3]. By contrast, transanal endoscopic platforms provide consistent exposure throughout the rectum, enabling surgeons to extend organ-preserving surgery far beyond what was previously achievable. These characteristics are particularly valuable when facing rare rectal tumours, where histological diagnosis is often uncertain preoperatively and an oncologically sound local excision may be both diagnostic and therapeutic[4].
The spectrum of rare lesions amenable to TEM and TEO is broad and heterogeneous, addressing conditions that develop both within and beyond the rectum[5]. Gastrointestinal stromal tumours (GISTs), neuroendocrine neoplasms (NENs), rectal melanoma, squamous cell carcinoma, and even metastatic lesions to the rectum represent oncological entities that require en bloc excision with negative margins for diagnosis and local control. In parallel, developmental and benign conditions such as duplication cysts, hamartomas, neuronal dysplasia, and heterotopias can also be excised with precision, thereby avoiding the morbidity associated with abdominal approaches. The ability of TEM and TEO to facilitate both full-thickness resections, ensuring accurate staging and margin clearance, as well as submucosal dissections, which preserve deeper structures when appropriate, exemplifies their adaptability to such diverse pathologies[6].
Equally important is the safety profile demonstrated by these platforms. Across indications, perioperative morbidity remains low, with peritoneal entry and postoperative bleeding representing the most frequent but manageable complications. Mortality directly attributable to TEM or TEO is exceedingly rare[7]. Hospitalisation is usually brief, often limited to only a few days, underscoring the minimal physiological burden of the approach. For patients with rare rectal lesions, many of whom are elderly or carry comorbidities, this reduced invasiveness is especially advantageous.
Despite their advantages, the application of TEM and TEO to rare indications has historically been under-reported. Most literature focuses on adenomas and early adenocarcinomas, which represent the bulk of clinical practice and have been extensively studied in terms of long-term oncological outcomes[8]. Reports of rarer entities are typically limited to case reports and small series, scattered across different disciplines. As a result, evidence regarding outcomes in these unusual settings remains fragmented, and clinicians often rely on extrapolation from more common indications. A systematic description of experience across multiple rare histologies, using a consistent platform and operative technique, is therefore of particular value to both surgeons and multidisciplinary teams.
Another crucial point is the role of TEM and TEO in organ preservation. Radical rectal resection carries substantial morbidity, including risks of anastomotic leakage, urinary and sexual dysfunction, and the potential need for permanent stoma formation[9]. In contrast, transanal endoscopic local excision avoids these burdens while still ensuring pathological diagnosis and local control. In an era where quality of life and functional preservation are increasingly recognised as key endpoints alongside oncological safety, the expansion of TEM and TEO into rare indications further consolidates their importance within rectal surgery.
METHODS
We conducted a retrospective observational cohort study at a single tertiary referral centre, examining consecutive patients who underwent local excision of rectal lesions with TEM or TEO between 1993 and 2024. Cases were identified from a prospectively maintained database. Inclusion criteria were: (i) local excision performed using TEM or TEO; (ii) definitive pathology showing a rare rectal lesion; and (iii) availability of core perioperative and follow-up data. Exclusion criteria were: (i) standard indications such as rectal adenomas or adenocarcinomas; (ii) non-rectal lesions; and (iii) incomplete records preventing outcome assessment. For clarity of reporting, pathologic reports were grouped a priori into the following categories: GIST, neuroendocrine tumours (NETs), neuroendocrine carcinomas (NECs), ulcerative solitary rectal syndrome (USR), hamartoma, duplication cyst, neuronal dysplasia combined with schwannoma, leiomyoma combined with leiomyosarcoma, squamous cell carcinoma combined with nodal metastasis from squamous carcinoma, gastric heterotopia, and melanoma. For each patient, we collected demographics, lesion size and site, operative details (including platform, resection plane, patient positioning, peritoneal entry, conversion, and resection margins), and postoperative outcomes (including complications, length of stay, further intervention, and follow-up with recurrence). Data were drawn directly from the electronic registry, with verification against operative and pathology reports when required. We summarised lesion size as mean with range, whereas time-based outcomes are reported as median with interquartile range. No formal hypothesis testing was planned, as the study’s intent was descriptive and exploratory, focusing on rare entities.
RESULTS
GIST
Thirteen patients were treated for GIST, with a mean age of 59 years (range 46-77) and a slight male predominance. Lesions measured on average 4.2 cm (range, 2-10 cm) and were more often located anteriorly. Preoperative assessment typically included endoscopy with biopsy, along with staging using endoscopic ultrasound (EUS) and magnetic resonance imaging (MRI). Resection was performed by TEO in the vast majority of patients and consisted of full-thickness excision in 12 cases and submucosal dissection in 1 case. Patients were positioned in the lithotomy position in most cases and in the prone position in the remainder. One peritoneal entry occurred and was managed without conversion. No postoperative complications were recorded. Resection margins were negative in 12 patients, and 1 had an R1 resection. The median hospital stay was four days [interquartile range (IQR), 2-6 days]. The median follow-up was 60 months (IQR, 22-76 months). Two patients developed a local recurrence confirmed as GIST, while no other recurrences were observed.
NENs
NENs were classified into well-differentiated NETs and poorly differentiated NECs[10]. This distinction was applied in the analysis of our patient cohort.
The NET group consisted of thirteen patients with a mean age of 62 years (range, 46-76) and an even distribution between the genders. The mean lesion size was 3 cm (range 2-10), and the tumours were slightly more often posterior. Preoperative work-up comprised endoscopy with biopsy and staging by EUS and MRI. Excision was full-thickness in all patients. TEO was the most frequent technique, with two cases treated by TEM. Positioning was lithotomy in 8 patients and prone in 5. Two peritoneal entries were documented but did not lead to conversion. All resections achieved negative margins. The median length of stay was 2 days (IQR, 2-5 days). Median follow-up was 36 months (IQR, 26-48 months). One patient experienced a nodal recurrence diagnosed at 36 months, and underwent salvage total mesorectal excision. One additional postoperative complication was recorded; it did not require transfusion or reoperation, and management details were coded in the database.
One additional patient, a 77-year-old woman, was treated for a poorly differentiated NEC. She presented with a posterior lesion measuring 7 cm and underwent TEO with a submucosal dissection chosen according to tumour stratigraphy. She was positioned in lithotomy. Margins were negative, and there was no peritoneal entry or conversion to laparoscopy. Her hospital stay was 2 days, and she remained recurrence-free at 3 months of follow-up. No complications were recorded.
USR
Six patients presented with USR, with a mean age of 55 years (range, 27-84 years) and a predominance of females. The lesions were typically located anteriorly and had a mean diameter of 3.8 cm (range, 2-8 cm). Diagnostic evaluation consisted of endoscopy and biopsy with selective use of EUS or MRI to exclude neoplasia. Excision was full-thickness in five patients and submucosal in one. Four procedures were performed in TEM and two in TEO. Positioning was prone in five patients and lithotomy in one. No peritoneal entries or conversions were recorded, and all resections were R0. The median hospital stay was 2.5 days (IQR, 2-5 days). The median follow-up was 33 months (IQR, 17-49 months). Two postoperative complications occurred: one postoperative bleeding episode required transfusion and reoperation, whereas the other was recorded as an unspecified complication in the database. No recurrence was observed.
Hamartoma
Five patients had hamartomas, with a mean age of 41 years (range 13-72) and a predominance of females. Lesions averaged 3.8 cm (range 3-6) and were located in mixed positions. All patients underwent full-thickness excision, four by TEO and one by TEM. Three were positioned in lithotomy and two in prone. No peritoneal entries or conversions occurred. Margins were negative in 4 cases and positive in 1. The median hospital stay was 4 days (IQR, 3-6 days). Median follow-up was 36 months (IQR, 25-36 months). One postoperative complication was recorded but did not require transfusion or reoperation. No recurrences were documented.
Duplication cyst
Two patients aged 16 and 46 years presented with duplication cysts with a mean size of 4 cm. Both lesions were excised by TEO as full-thickness resections, with patients positioned in lithotomy. Margins were clear in both cases. There were no peritoneal entries or conversions. The median length of stay was 3 days (IQR, 2-4 days). The median follow-up was 4.5 months (IQR, 2-7 months). No complications or recurrences occurred.
Neuronal dysplasia and schwannoma
Two women, aged 45 and 53 years, underwent excision for these rare neurogenic lesions measuring between 2 and 6 cm. One procedure was performed in TEM and the other in TEO, both with full-thickness dissection. One patient was positioned in lithotomy and the other in prone. All resections were R0, and there were no peritoneal entries or conversions. The median length of stay was three days (IQR, 3-4 days). The median follow-up was 18 months (IQR, 9-26 months). No complications or recurrences were documented.
Leiomyoma and leiomyosarcoma
Two men, aged 43 and 51 years, presented with anterior lesions approximately 5 cm in diameter. Both were excised with full-thickness dissection, one in TEM and one in TEO, with both patients positioned in the prone position. Resection margins were negative, and there were no peritoneal entries or conversions. The median length of stay was five days (IQR, 4-6 days). Median follow-up was 10 months. No complications or recurrences were reported.
Squamous cell carcinoma and nodal metastasis from squamous carcinoma
Two patients, with a mean age of 76 years (range, 69-82 years), presented with anterior lesions approximately 3 cm in diameter. Both were treated with full-thickness excision by TEO. One was positioned prone, and the other in lithotomy. Margins were negative, and no peritoneal entries or conversions were observed. The median hospital stay was 2.5 days (IQR, 2-3 days). Median follow-up was 36 months. No complications were documented. One patient developed a distant recurrence at 12 months.
Gastric heterotopia
A 62-year-old man was treated for a 2 cm posterior lesion, excised by TEM with full-thickness dissection in lithotomy position. Margins were clear, and no peritoneal entry or conversion was required. He remained hospitalised for 4 days, and no complications were noted. No follow-up data were available in the dataset, and no recurrence was recorded.
Melanoma
A 78-year-old woman presented with a 5 cm anterior lesion. She underwent TEO with full-thickness dissection in the prone position. Margins were negative, and no peritoneal entry or conversion occurred. Her hospital stay was five days, and she remained without events at database closure.
Patient characteristics and the main perioperative and follow-up outcomes are presented in Table 1. Intraoperative variables and perioperative complications are outlined in Table 2.
Characteristics of patients by histological subgroup
| Histology subgroup | N | Lesion size, cm (mean [range]) | Operative time, min (median [IQR]) | Anaesthesia (general/spinal) | Length of stay, days (median [IQR]) | Margins (R0/R1) | Any complication (n) | Any recurrence (n) |
| GIST | 13 | 4.2 [2-10] | 80 [60-110] | 4/9 | 4 [2-6] | 12/1 | 0 | 2 |
| NEN - NET - NEC | 13 1 | 3 [2-10] 7 [7-7] | 52 [37-80] 80 | 4/9 1/0 | 2 [2-5] 2 | 13/0 1/0 | 1 0 | 1 0 |
| USR | 6 | 3.8 [2-8] | 60 [50-90] | 6/0 | 2.5 [2-5] | 6/0 | 2 | 0 |
| Hamartoma | 5 | 3.8 [3-6] | 65 [55-80] | 5/0 | 4 [3-6] | 4/1 | 1 | 0 |
| Duplication cyst | 2 | 4 [4-4] | 55 [50-60] | 2/0 | 3 [2-4] | 2/0 | 0 | 0 |
| Neuronal dysplasia/schwannoma | 2 | 4 [2-6] | 65 [60-70] | 2/0 | 3 [3-4] | 2/0 | 0 | 0 |
| Leiomyoma/leiomyosarcoma | 2 | 5 [5-5] | 70 [65-75] | 2/0 | 5 [4-6] | 2/0 | 0 | 0 |
| SCC/nodal metastasis | 2 | 3 [3-3] | 60 [55-65] | 2/0 | 2.5 [2-3] | 2/0 | 0 | 1 |
| Gastric heterotopia | 1 | 2 [2-2] | 50 | 1/0 | 4 | 1/0 | 0 | 0 |
| Melanoma | 1 | 5 [5-5] | 80 | 1/0 | 5 | 1/0 | 0 | 0 |
Intraoperative variables and perioperative complications
| Histology subgroup | N | Dissection plane, full/submucosal | Positioning, lithotomy/prone | Peritoneal entry, n |
| Duplication cyst | 2 | 2/0 | 2/0 | 0 |
| GIST | 13 | 12/1 | 9/4 | 1 |
| Gastric heterotopia | 1 | 1/0 | 1/0 | 0 |
| Hamartoma | 5 | 5/0 | 3/2 | 0 |
| Leiomyoma + leiomyosarcoma | 2 | 2/0 | 0/2 | 0 |
| Melanoma | 1 | 1/0 | 0/1 | 0 |
| NEN - NET - NEC | 13 1 | 13/0 0/1 | 8/5 1/0 | 2 0 |
| Neuronal dysplasia + schwannoma | 2 | 2/0 | 1/1 | 0 |
| SCC + nodal SCC metastasis | 2 | 2/0 | 1/1 | 0 |
| USR | 6 | 5/1 | 1/5 | 0 |
DISCUSSION
This study demonstrates that transanal endoscopic platforms provide a practical and versatile approach for the excision of rare rectal lesions, with favourable safety and oncological profiles. It should be stressed that TEM and TEO represent surgical platforms rather than procedures in themselves. The distinction is essential, as the platforms are designed to offer a stable pneumorectum, precise instrumentation, and magnified vision, which can then be employed to perform different types of dissection according to the pathology and the surgeon’s intent. The procedure is therefore defined not by the platform, but by the dissection plane and the surgical strategy undertaken.
In this cohort, both full-thickness and submucosal dissections were undertaken, each chosen according to the biological behaviour and expected depth of the lesion. Full-thickness resection was performed in the overwhelming majority of patients, particularly where diagnostic certainty was required or where oncological adequacy was paramount. Submucosal dissection was reserved for lesions in which the pathology or imaging suggested confinement to the mucosa or superficial submucosa. The availability of both strategies within the same platform underscores the adaptability of TEM and TEO. Compared with conventional transanal excision, TEM has consistently been associated with better specimen quality, higher R0 rates, and lower local recurrence in rectal lesions, and these same technical advantages likely explain its performance in uncommon histologies[2,3,11].
Oncological adequacy is a central consideration in the treatment of rare rectal tumours[12], many of which pose unique biological challenges. In this series, clear resection margins were achieved in nearly all patients, with only a handful of R1 resections. Recurrence was exceptional, and when it did occur, it was documented several years later, underscoring that local control is reliably achievable when these platforms are employed. These findings align with larger series reporting high R0 rates for more common indications, such as adenomas and early adenocarcinoma, where TEM and TEO consistently outperform conventional transanal surgery in terms of margin status and recurrence rates[6]. The current data extend this principle into much rarer histologies, including GIST, NEN, melanoma, squamous carcinoma, and hamartomas, confirming the broad utility of the approach[13-15].
Complications were infrequent and generally minor. The most common intraoperative issue, peritoneal entry, occurred in only three patients and was always manageable within the platform without conversion to open or laparoscopic surgery. Overall postoperative morbidity comprised four events: one bleeding episode requiring transfusion and reoperation and three additional non-fatal complications recorded in the database. Mortality was nil. This confirms the widely accepted safety profile of transanal endoscopic surgery, which is characterised by extremely low rates of significant complications and minimal physiological stress on the patient[16]. In addition, the length of stay was very short, with a median of two to five days across all subgroups, reflecting both the minimally invasive nature of the intervention and the rapid recovery it affords. This stands in stark contrast to abdominal resections, which, even in modern laparoscopic series, still require longer hospitalisation, higher morbidity, and a greater risk of stoma formation[17].
The rarity of the lesions presented here deserves particular attention. By their very nature, tumours such as rectal GIST, NEN, duplication cysts, or rectal melanoma are seldom encountered in clinical practice, which makes drawing generalisable conclusions difficult. However, the present series confirms that the platform-based strategy is robust across a heterogeneous range of histologies. The ability to maintain margin negativity, avoid conversion, and minimise complications across this spectrum supports the idea that TEM and TEO can be considered the standard rigid transanal endoscopic platforms for rare rectal lesions when local excision is deemed appropriate. This has implications for centres that may otherwise consider such lesions unsuitable for transanal management, potentially expanding organ-preserving options for patients. Beyond rare histotypes, the versatility of these platforms is also illustrated by atypical indications reported in the literature, such as treatment of complete rectal prolapse using the TEO platform[18].
Another important point concerns the learning curve and dissemination of the technique. TEM has historically been associated with a steep learning curve, partly due to the rigid rectoscope and dedicated instruments. TEO was developed to provide a shorter, more accessible system with a high-definition camera and more ergonomic handling[19]. Both platforms, however, offer the same essential benefits of stability and magnification. The rarity of the cases in this series suggests that centres must maintain broad expertise and a culture of multidisciplinary discussion to integrate these rare pathologies into practice. Training curricula are increasingly incorporating simulation and structured assessment, and the application of these tools to TEM and TEO will likely further shorten the learning curve and ensure the reproducibility of outcomes[20].
From a comparative perspective, alternative methods exist for the local excision of rectal lesions, most notably transanal minimally invasive surgery (TAMIS) and endoscopic submucosal dissection (ESD). TAMIS utilises a disposable transanal port and laparoscopic instruments, offering flexibility and ease of setup. However, its stability and visualisation are often inferior to TEM and TEO, particularly for more proximal lesions[21]. ESD, on the other hand, is a purely endoscopic approach that excels in mucosal and superficial submucosal lesions but is less reliable for full-thickness resections and cannot provide the same degree of control once the muscularis propria is entered. Nevertheless, the superiority of one device over the other for mucosal lesion is still under discussion[22]. For rare tumours with uncertain behaviour or need for definitive histological staging, TEM and TEO therefore remain the gold standard, bridging the gap between minimal invasiveness and oncological adequacy.
Limitations of the present study must be acknowledged. The data derive from a retrospective series spanning over 20 years of surgical activity, and which is susceptible to information bias and missing data. Follow-up was heterogeneous, with some patients followed for many years and others censored shortly after surgery. The rarity of the lesions means that numbers are small in each subgroup, limiting the ability to detect infrequent outcomes. Moreover, detection of recurrence was based on clinical records rather than a protocolised surveillance programme, which may underestimate true incidence. Nonetheless, the strengths include the consecutive nature of the series, the prospective maintenance of the database, and the detailed operative documentation, which provide a reliable description of practice and outcomes in this unusual setting.
Looking to the future, new technologies may further extend the scope of transanal platforms. Robotic assistance has already been applied in the form of robotic TAMIS and robotic-assisted TEO, offering improved dexterity, three-dimensional vision, and potentially more precise suturing[23]. Whether these advantages translate into measurable clinical benefits for rare lesions remains to be established, but early reports suggest feasibility and safety. Similarly, flexible transanal platforms are under development, which may combine the advantages of endoscopic manoeuvrability with the stability of rigid systems. Artificial intelligence and computer vision may also play a role in enhancing safety and training by providing real-time feedback on dissection planes, instrument handling, and error recognition[24]. These innovations may ensure that even the rarest rectal tumours can be managed with increasing consistency and safety.
In conclusion, the present findings reinforce the broader principle of organ preservation in rectal surgery. Although the numbers are small, the capacity to manage unusual tumours with low morbidity, nil mortality, and rapid recovery supports the philosophy of avoiding unnecessary radical resections when a safe and oncologically adequate local excision can be achieved. For patients, this means not only reduced operative risk but also preservation of bowel function and quality of life, outcomes that are particularly valuable in a population often facing complex oncological decisions. The challenge for the surgical community is to ensure that such opportunities are not missed due to a lack of familiarity or access to the appropriate platforms.
DECLARATIONS
Authors’ contributions
Study conception and design: Arezzo A, Distefano G, Morino M
Data acquisition: Arezzo A, Distefano G, Ammirati CA, Barbiero M
Data analysis and interpretation: Arezzo A, Distefano G, Morino M
Drafting of the manuscript: Arezzo A, Distefano G
Critical revision of the manuscript for important intellectual content: Arezzo A, Distefano G, Ammirati CA, Barbiero M, Morino M
All authors approved the final version of the manuscript to be published.
Availability of data and materials
All data generated or analysed during this study are included in this published article. Additional data related to this study are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool Grammarly (version 9.98.0, released 2026-06-04) was used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This work was supported by the European Research Council (ERC) under the Horizon Europe programme (Grant EndoTheranostics, Grant Agreement No. 101118626, DOI: 10.3030/101118626), the CLASSICA project (Grant Agreement No. 101057321, DOI: 10.3030/101057321) and the PALPABLE project (Grant Agreement No. 101092518, DOI: 10.3030/101092518). The work has also been partially supported by the Italian Ministry of University and Research (MUR) under the PRIN 2022 programme “Towards Intelligent ROBOTIC ENDOSCOPIC DISSECTION (TI-RED)”. Views and opinions expressed are, however, those of the author(s) only and do not necessarily reflect those of the European Union, the European Research Council Executive Agency, or the Health and Digital Executive Agency. Neither the European Union nor the granting authority can be held responsible for them.
Conflicts of interest
Arezzo A and Morino M are Editorial Board Members of the journal Mini-Invasive Surgery. They were not involved in any part of the editorial process for this manuscript, including reviewer selection, manuscript handling, or decision-making. The other authors declare that they have no conflicts of interest.
Ethical approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. As this was a retrospective observational study based exclusively on de-identified/anonymised data collected during routine clinical practice, with no experimental intervention, no modification of patient management, and no additional diagnostic or therapeutic procedures; prior Ethics Committee approval was not required according to applicable Italian regulations and institutional procedures. Individual informed consent was not required for the retrospective analysis of previously collected de-identified data for scientific research purposes under Italian legislation governing health-related data, including Article 110 of Legislative Decree no. 196/2003, as amended, and Regulation (EU) 2016/679.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Buess G, Kipfmüller K, Hack D, Grüssner R, Heintz A, Junginger T. Technique of transanal endoscopic microsurgery. Surg Endosc. 1988;2:71-5.
2. Winde G, Blasius G, Herwig R, Lügering N, Keller R, Fischer R. Benefit in therapy of superficial rectal neoplasms objectivized: transanal endoscopic microsurgery (TEM) compared to surgical standards. Minim Invasive Ther Allied Technol. 1997;6:315-23.
3. Moore JS, Cataldo PA, Osler T, Hyman NH. Transanal endoscopic microsurgery is more effective than traditional transanal excision for resection of rectal masses. Dis Colon Rectum. 2008;51:1026-30; discussion 1030.
4. Arezzo A, Arolfo S, Cravero F, Migliore M, Allaix ME, Morino M. Which treatment for large rectal adenoma? Preoperative assessment and therapeutic strategy. Minim Invasive Ther Allied Technol. 2014;23:21-7.
5. Duek SD, Gilshtein H, Khoury W. Transanal endoscopic microsurgery: also for the treatment of retrorectal tumors. Minim Invasive Ther Allied Technol. 2014;23:28-31.
6. Arezzo A, Passera R, Saito Y, et al. Systematic review and meta-analysis of endoscopic submucosal dissection versus transanal endoscopic microsurgery for large noninvasive rectal lesions. Surg Endosc. 2014;28:427-38.
7. Middleton PF, Sutherland LM, Maddern GJ. Transanal endoscopic microsurgery: a systematic review. Dis Colon Rectum. 2005;48:270-84.
8. Morino M, Allaix ME. Transanal endoscopic microsurgery: what indications in 2013? Gastroenterol Rep. 2013;1:75-84.
9. Heald RJ, Moran BJ, Ryall RD, Sexton R, MacFarlane JK. Rectal cancer: the Basingstoke experience of total mesorectal excision, 1978-1997. Arch Surg. 1998;133:894-9.
10. Nagtegaal ID, Odze RD, Klimstra D, et al.; WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020;76:182-8.
11. Park SS, Kim BC, Lee DE, et al. Comparison of endoscopic submucosal dissection and transanal endoscopic microsurgery for T1 rectal neuroendocrine tumors: a propensity score-matched study. Gastrointest Endosc. 2021;94:408-15.e2.
12. Gronchi A, Bonvalot S, Poveda Velasco A, et al. Quality of surgery and outcome in localized gastrointestinal stromal tumors treated within an international intergroup randomized clinical trial of adjuvant imatinib. JAMA Surg. 2020;155:e200397.
13. Shi WK, Hou R, Li YH, et al. Long-term outcomes of transanal endoscopic microsurgery for the treatment of rectal neuroendocrine tumors. BMC Surg. 2022;22:43.
14. Guaglio M, Belli F, Cesa Bianchi A, Sorrentino L, Battaglia L. Minimizing the surgical approach for a rare disease: transanal endoscopic microsurgery for rectal schwannoma. Tumori. 2019;105:NP52-6.
15. Punnen S, Karimuddin AA, Raval MJ, Phang PT, Brown CJ. Transanal endoscopic microsurgery (TEM) for rectal GI stromal tumor. Am J Surg. 2021;221:183-6.
16. De Graaf EJ, Doornebosch PG, Tollenaar RA, et al. Transanal endoscopic microsurgery versus total mesorectal excision of T1 rectal adenocarcinomas with curative intention. Eur J Surg Oncol. 2009;35:1280-5.
17. Kethman WC, Harris AHS, Morris AM, Shelton A, Kirilcuk N, Kin C. Oncologic and perioperative outcomes of laparoscopic, open, and robotic approaches for rectal cancer resection: a multicenter, propensity score-weighted cohort study. Dis Colon Rectum. 2020;63:46-52.
18. D’Urso A, Lapergola A, Marescaux J, Mutter D, Serra-Aracil X. Treatment of complete rectal prolapse using the TEO® platform (transanal endoscopic operation) - a video vignette. Colorectal Dis. 2024;26:820-2.
19. Hur H, Bae SU, Han YD, et al. Transanal endoscopic operation for rectal tumor: short-term outcomes and learning curve analysis. Surg Laparosc Endosc Percutan Tech. 2016;26:236-43.
20. Boland PA, McEntee PD, Murphy E, et al. Local excision of rectal neoplasia: a real-world survey of current practices and perspectives. Minim Invasive Ther Allied Technol. 2025;34:335-43.
21. Chavda V, Siaw O, Chaudhri S, Runau F. Management of early rectal cancer; current surgical options and future direction. World J Gastrointest Surg. 2021;13:655-67.
22. Kouladouros K, Warkentin V, Kähler G. Transanal endoscopic microsurgical submucosal dissection: are there advantages over conventional ESD? Minim Invasive Ther Allied Technol. 2022;31:720-7.
23. Marks JH, Perez RE, Salem JF. Robotic transanal surgery for rectal cancer. Clin Colon Rectal Surg. 2021;34:317-24.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].